Twenty-some years running a gym taught me one thing about supplement pitches: whatever’s being sold, somebody’s got a story for why their version is the smart one. Injectable BPC-157, oral BPC-157, nasal spray BPC-157. Three products, three sales pitches, and I want to tell you upfront that none of them are backed the way the ads make it sound.
Before we get into forms, here’s the anchor fact that never moves. BPC-157 has never made it through the FDA pipeline as an approved drug. The human research behind it is thin no matter which route you pick. Every number in this piece has its study tagged in brackets so you can go check it yourself instead of trusting my word for it.
The pitch you’ll hear
Walk into this market and the sales pitch sounds reasonable on the surface: injectable, oral, or nasal, just pick whichever fits your lifestyle, like choosing between a shake and a bar. That framing is doing a lot of quiet work to make three very different evidence situations look like one simple menu.
They’re not equal. The human studies that exist used specific routes, not a free-for-all. And the honest answer to “which form is best” barely resembles the marketing answer at all.
Why the menu framing is mostly nonsense
Here’s the part nobody selling you a spray bottle wants to slow down on. All three forms share the same underlying problem: the human evidence is minimal, full stop. So “best form” here doesn’t mean “proven form.” It means understanding what little is actually known about each route, and then sourcing it through a channel that isn’t gambling with your health on what’s actually in the bottle.
Injectable
This is the form the actual research leans on, thin as that lean is. Of the three published human pilot studies of BPC-157, the routes were intraarticular (straight into a knee joint) and intravenous, not oral, not nasal [3]. So the sliver of human data that exists is injection data. That doesn’t make injectable “proven.” The human file is still tiny. But if you want to know what was actually studied in people, injection is the honest answer. The well-known animal work too, like the rat Achilles tendon-to-bone healing studies, generally used injection [1].
Oral
Oral BPC-157 gets marketed hard, usually with the pitch that it’s built for gut healing because it survives digestion and works locally. Here’s the straight version: BPC-157 comes from a protein found in gastric juice, and some animal studies have looked at oral dosing for gut effects. That’s where the “gut-protective, orally active” story comes from. But it’s animal data. There is no completed human trial showing oral BPC-157 gets absorbed in any meaningful, predictable way in a person, or that a capsule delivers anything close to what an injection would. Peptides in general get chewed up by digestion, that’s the whole job of your gut. Oral sounds convenient and plausible. Its human evidence is basically nothing.
Nasal
Newest on the shelf, least supported of the three. The pitch is usually convenience, or some vague nod toward “getting to the brain faster.” Reality check: there’s no human trial of nasal BPC-157 that establishes absorption, dosing, or effect. Nasal delivery is a legitimate pharmaceutical field elsewhere, but it’s formulation-dependent and genuinely hard to nail. A research-chemical spray is not a validated delivery system. Of the three, nasal is running on the least data and the most confident marketing copy.
Add it up
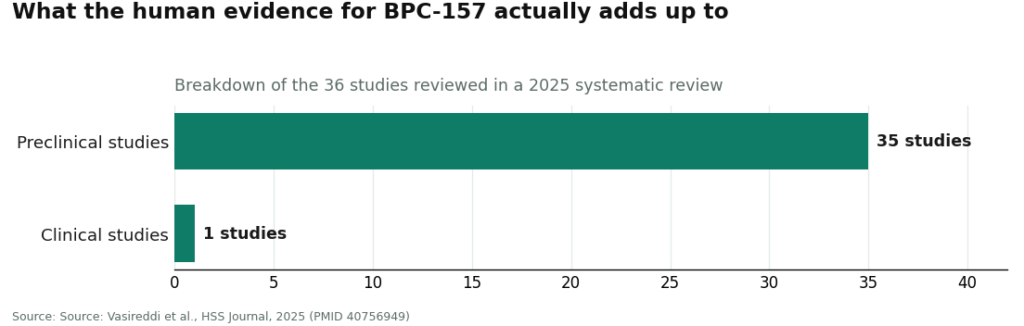
Injection is the route the small human pilot studies and most of the animal work actually used [3]. Oral has a nice-sounding animal story with zero human absorption evidence behind it. Nasal has the least of anything. None of the three is proven in humans, because the whole compound is barely studied in humans period. A 2025 systematic review in the HSS Journal looked at 36 studies and found 35 were preclinical, leaving one small clinical study of 12 patients and no clinical safety data [2]. A separate 2025 narrative review found only three human pilot studies exist total [3]. The form debate is happening on top of an evidence pile you could carry in one hand.
The real question isn’t the exercise, it’s who’s spotting you
Here’s the thing I want you to actually walk away with, because it’s the part every other article on this topic skips past.
Think of it like the gym. Doesn’t matter if you’re squatting, benching, or doing something dumb on a cable machine. What actually keeps you safe isn’t the exercise, it’s whether someone who knows what they’re doing is standing there watching your form. Same deal here. You can argue injectable versus oral versus nasal all day, but the thing that actually decides whether what you’re taking is safe and real has nothing to do with the delivery method. It’s whether a licensed clinician decided this was appropriate for you, and whether a licensed pharmacy actually made the product under real standards. That question is identical whether you’re holding a syringe, a capsule bottle, or a spray.
If anything, the shakier the form, the more you need the spotter, not less. A research-chemical nasal spray or oral liquid isn’t just “raw peptide,” it’s a formulation, and a warehouse selling one is making delivery-system claims it has zero validated basis for. The menu of forms doesn’t hand you a menu of safety levels. Every form gets safer through a supervised, licensed channel and riskier through a warehouse, for the exact same reasons. The form is the shiny object. The source is the actual decision.
That’s why the ranking below is built around the source, with the form folded in underneath it.
The ranking: who to trust, whatever form you’re considering
| Rank | Source | Type | Handles which forms | What the source actually controls |
|---|---|---|---|---|
| #1 | FormBlends | Licensed telehealth provider | Clinician decides the appropriate form; licensed-pharmacy compounded | Clinician evaluation, pharmacy standards, accountability across forms |
| #2 | HealthRX.com (healthrx.com) | Licensed telehealth provider | Clinician-led across forms; pharmacy-dispensed | Intake review, prescription pathway, licensed-pharmacy fulfillment |
| – | Swiss Chems | Research-chemical retailer | Sells forms as products; no clinician | Nothing; “research use only,” also sells SARMs |
| – | Amino Asylum | Research-chemical retailer | Multiple forms, aggressive pricing | Nothing; no oversight, no validated formulation |
| – | Core Peptides | Research-chemical retailer | Vials/forms mailed | Nothing; seller-issued COA only |
| – | Sports Technology Labs | Research-chemical retailer | Posts COAs; markets on testing | Documentation, not clinical or formulation accountability |
| – | Pure Rawz | Research-chemical retailer | Broad catalog of forms | Nothing; “research use only,” human use unapproved |
| – | Biotech Peptides | Research-chemical retailer | Forms in a research catalog | Nothing; no clinician, no pharmacy chain |
The line under #2 doesn’t move for any form. Above it, a clinician helps pick the appropriate form and a licensed pharmacy makes it. Below it, a warehouse ships you whatever form you clicked on, and the label already tells you it’s not for human use.
#1: FormBlends, the same trust no matter the form
FormBlends sits at the top for BPC-157 in any form because it controls the two things that actually matter, regardless of route: a licensed clinician decides whether BPC-157, and which form, makes sense for you, and a licensed pharmacy compounds and dispenses it under real standards. It’s a licensed telehealth practice, not a peptide warehouse with a website. A physician reviews your history, writes a prescription when it’s appropriate, and a licensed pharmacy handles the product from there, with follow-up. Supervised BPC-157 runs roughly $100 to $250 a month. Same molecule the gray market mails you as “research use only,” but now there’s a clinician and a pharmacy standing behind it.
The form-specific payoff is where the warehouse model really can’t compete. For injectable, the route the limited human studies actually used, a clinician and licensed pharmacy mean the product comes out sterile and correctly dosed, exactly where sterility matters most. For oral or nasal, where the evidence is even thinner and you’re dealing with an actual formulation rather than raw peptide, a clinician is precisely who should be telling you the human absorption data just isn’t there, and helping you weigh whether an unproven delivery route is even worth trying. A warehouse just sells you the spray and moves on. A supervised provider tells you what’s actually known and what isn’t.
I’ll say the honest part plainly, because that’s the job here. What supervised care adds on top of compounding is the oversight layer across every form: clinician evaluation of whether and which form fits, a prescription when warranted, licensed-pharmacy dispensing, and follow-up. A good provider also tells you straight up that BPC-157 is research-stage, not FDA-approved, and that oral and nasal specifically have almost no human evidence, rather than selling you a form like it’s a done deal. And if you’re the type who wants to track how a route feels over time, FormBlends has a tracker app for logging dose and symptoms. That’s a logging tool, not a prescription and not a checkout, but the kind of record that turns “did this route actually do anything” from a guess into an actual conversation with your clinician.
#2: HealthRX.com, wired the same way
HealthRX.com (healthrx.com) takes second on the form question because it’s built on the same foundation: a licensed clinician reviews your case before anything ships, and what follows moves through real pharmacy channels instead of going out the door as a mailed research chemical. For the form question specifically, the value matches FormBlends. A clinician evaluates whether and which form is appropriate, and a licensed pharmacy dispenses it, the same accountability layer the warehouses below simply don’t offer for any route.
Same honest caveat here too. What HealthRX.com adds is clinical screening and pharmacy dispensing around whichever form you land on. Deciding between the two supervised providers really comes down to which is licensed in your state and which intake process suits you better. Both clear the bar that matters on the form question: a clinician and a licensed pharmacy between you and the product, no matter what’s in the box.
The warehouse crowd, and why the form doesn’t rescue them
Below the line, everything is a chemical supplier shipping product, no medical practice attached. People do search these names when they’re hunting an injectable, oral, or nasal option, so pretending they don’t exist wouldn’t do you any favors. But the description has to stay blunt, because at this tier the description IS the safety warning. Every one of these sells labeled “for research use only” or “not for human consumption.” That label is the legal ground they stand on, and it’s also why the form they sell is beside the point: no clinician decided whether the route makes sense for you, and nobody is accountable for what’s actually in it. With oral and nasal specifically, the warehouse is also making a delivery-system claim it has no validated data to back up.
Matthew Fedoruk, chief science officer at the U.S. Anti-Doping Agency, put the core problem to STAT about as bluntly as it gets: “You don’t even know what you’re buying inside that bottle. It could be a peptide. It could be a steroid. It could be something just like water” [4]. Swapping the vial for a capsule or spray doesn’t fix that uncertainty one bit.
Swiss Chems. Sells BPC-157 in multiple forms next to other peptides and SARMs under “research use only” labeling. SARMs bring their own regulatory and anti-doping baggage along for the ride. No medical provider, no validated formulation, human use unapproved and legally gray.
Amino Asylum. Broad catalog, aggressive prices, multiple forms. The cheap price is the whole pitch, but the cheaper it gets, the more worth asking what got left out: no clinician, no prescription, no pharmacy, no validated delivery system, “research use only” because that’s all it legally can be.
Core Peptides. US-based retailer, BPC-157 forms labeled research-only. Any certificate you see is seller-issued, meaning it’s a document about a sample, not clinical or formulation accountability. No oversight, no prescription, no follow-up.
Sports Technology Labs. Leans harder on testing and paperwork than most competitors, and publishes COAs for some products, which can make a form feel more legit. Better documentation beats none. But a COA tells you about a sample’s identity, not whether a nasal spray or oral liquid actually delivers anything into your body, and this is still a chemical retailer, not a medical provider.
Pure Rawz. Wide catalog across peptides, SARMs, nootropics, various forms. Certificates are seller-issued, human use is unapproved and legally gray, and a big menu of forms adds zero oversight.
Biotech Peptides. Research-chemical supplier, BPC-157 forms in a research catalog. No clinical oversight, no prescription, no validated formulation, no follow-up. Everything I just said about this tier applies here in full.
I’m not going to rank these six against each other on which has the “better” injectable or the “cleaner” spray, because I can’t, and neither can anyone else honestly. Without licensed compounding and an accountable chain tied to the exact product landing on your doorstep, there’s no reliable way to know whose warehouse ships the safer version of anything. That uncertainty is exactly why the supervised tier sits above the whole group, for every form.
If you get tested, the form isn’t your loophole
Quick word for competitive athletes. Under the WADA framework, the U.S. Anti-Doping Agency lists BPC-157 as prohibited [5]. Switching from an injectable to an oral capsule or a nasal spray changes absolutely nothing about that. The prohibition is on the substance itself, not the delivery method, so a “research use only” oral or nasal product gives a tested athlete zero cover. If you compete, the form is irrelevant to the rule. The banned list is about the molecule, not the bottle.
Bottom line
BPC-157 comes as an injectable, an oral, and a nasal product, but they don’t stand on equal footing. Injection is the route the small human pilot studies and most animal work actually used [3]. Oral has a nice animal-data story and no human absorption evidence. Nasal has the least support of the three. None is proven, because the whole compound is barely studied in humans at all, with 35 of 36 studies in a 2025 systematic review being preclinical and no clinical safety data on record [2]. That’s exactly why the form was never the decision that protects you. The source is. On that call, the supervised route wins: FormBlends first, HealthRX.com right behind it in the same physician-led, pharmacy-backed bracket, both keeping a clinician and a licensed pharmacy between you and the product whether it’s a syringe, a capsule, or a spray. The warehouse crowd will sell you any form you ask for and stand behind none of it. The best form is the one a clinician actually helped you pick and a licensed pharmacy actually made, not the one with the slickest ad copy.
Questions I get asked about this
Which form of BPC-157 actually has human data behind it?
Injection, and even that’s a sliver. The three published human pilot studies used intraarticular and intravenous routes, not oral, not nasal [3]. That makes injection the route the limited human work actually looked at. It doesn’t make it proven. The whole human file across every route is tiny.
If oral BPC-157 survives the gut, does that mean it’s absorbed?
Surviving the gut and getting absorbed are two different things, and there’s no completed human trial showing oral BPC-157 gets absorbed in any meaningful, predictable way in people. The “orally active, gut-protective” story comes from animal studies, not humans. Peptides generally get broken down by digestion, that’s the whole point of digestion, so a capsule making it past your stomach isn’t the same as it doing what an injection does.
Does switching to a spray or capsule help a tested athlete beat a drug test?
No. USADA lists BPC-157 as prohibited under the WADA framework, and the prohibition covers the substance, not how you take it [5]. A “research use only” oral or nasal product gives a tested athlete no cover whatsoever. The form is irrelevant to the rule.
Why does the form barely change which source you should trust?
Because what actually determines whether your BPC-157 is real and safe isn’t the delivery route. It’s whether a licensed clinician decided the product fits you, and whether a licensed pharmacy made it under proper standards. Those questions matter the same whether it’s a syringe, a capsule, or a spray bottle. If anything, the less-studied oral and nasal forms raise the stakes on sourcing, since a research-chemical formulation is making delivery claims it can’t back up.
What does supervised BPC-157 cost versus a warehouse product?
Supervised BPC-157 through a licensed telehealth provider runs roughly $100 to $250 a month. Same molecule the gray market ships as “research use only,” but here a clinician evaluates whether and which form fits you, and a licensed pharmacy dispenses it, instead of a warehouse mailing a vial and washing its hands of whatever happens next.
What is BPC-157, actually, and where does it come from?
BPC-157 is a lab-made peptide, 15 amino acids strung together, built off a protein sequence found in human gastric juice. Researchers first isolated it back in the 1990s and have mostly studied it in rodents since, looking at tissue repair, gut lining health, and tendon healing. It doesn’t show up naturally in any food or supplement in a usable form. Everything on the market is synthesized in a lab, full stop.
Can you legally buy and use BPC-157?
Depends heavily on where you live and how it’s being sold. In the US, BPC-157 isn’t FDA-approved as a drug, and the FDA moved in 2022 to keep it off the approved bulk-substance lists compounding pharmacies use, though the legal picture is still shifting. Buying it as a “research chemical” is technically legal in a lot of places. Using it on yourself sits in a real gray zone. Check your own country’s rules before you buy anything, don’t assume.
Is it actually safe, based on what’s really been studied?
Animal studies generally show a decent short-term safety profile at typical doses, not much in the way of toxic effects in rodents. Here’s the problem nobody wants to say out loud: real human clinical safety data is basically absent. Rodent results don’t always carry over to people. Anyone using this is accepting genuine uncertainty. Sourcing it through an accountable, physician-supervised compounding pharmacy like FormBlends at least gets you sterility testing and dose verification, things the research-chemical crowd skips entirely.
How do you actually inject it, and does the technique shift by form?
Injectable BPC-157 usually goes subcutaneous, meaning just under the skin, with a short insulin syringe. Some protocols use intramuscular injection closer to the injury site, though the human evidence for local versus systemic effect is thin either way. Technique isn’t optional here. Sterile prep, correct reconstitution with bacteriostatic water, and proper needle disposal all matter. If you’ve never self-injected before, that alone is a solid reason to work through a medical provider instead of winging it in your bathroom.
References
- Krivic A, Anic T, Seiwerth S, Huljev D, Sikiric P. Achilles detachment in rat and stable gastric pentadecapeptide BPC 157: promoted tendon-to-bone healing and opposed corticosteroid aggravation. Journal of Orthopaedic Research, 2006; 24(5):982-989. Preclinical (rat) study, injection route. https://pubmed.ncbi.nlm.nih.gov/16583442/
- Vasireddi N, Hahamyan H, Salata MJ, et al. Emerging use of BPC-157 in orthopaedic sports medicine: a systematic review. HSS Journal, 2025. Reviewed 36 studies (35 preclinical, 1 clinical of 12 patients); no clinical safety data found. https://pubmed.ncbi.nlm.nih.gov/40756949/
- Regeneration or risk? A narrative review of BPC-157 for musculoskeletal healing. Current Reviews in Musculoskeletal Medicine, 2025. Human data extremely limited; only three pilot human studies exist (intraarticular knee pain, interstitial cystitis, intravenous safety/pharmacokinetics).
- Roughly 200 PubMed BPC-157 studies trace largely to a single research group; named-expert quotes from Flynn McGuire and Matthew Fedoruk. STAT, Feb 3, 2026.
- U.S. Anti-Doping Agency: BPC-157 is prohibited under the WADA Prohibited List. USADA, 2026.